
Serious Mental Illness is an Optimization Problem
Contra Scott Alexander on Mentally Ill Homeless People

Over at Astral Codex Ten, psychiatrist and pseudonymous blogger Scott Alexander has a recent piece on the challenges of dealing with “mentally ill homeless people.” I think it is not unfair to say that Alexander’s argument is, in essence, that the status quo is about as good as we can get, and that people claiming otherwise are often not explaining how to get to better, rather than simply suggesting that better must be possible.
I am sympathetic to the meta-point: “things ought to be better!” is an irritating refrain to hear from people who do not work in your area of expertise and assume that policy failures are failures of will, rather than products of constraints. But the fact that Alexander is a practitioner in this space—that he has a micro view—does not mean that he has any particular grasp on the macro realities of mental health policy. And I think the situation he regards as intractable is actually entirely tractable. The constraints are not intrinsic, but ideological: we simply do not do enough to prioritize the well-being of the seriously mentally ill.
First, let me review Alexander’s argument. As he explains it, the current approach to “disruptive mentally ill homeless people” is that they are identified; arrested; committed to a hospital with a psych ward; put on antipsychotics; allowed to stabilize; and released, at which point the entire cycle begins again. I have no reason to contest this account, as it basically jives with my understanding of SOP in most American jurisdictions.
One simple way to think about this approach is that it intervenes only when and insofar as a person is in crisis—when his untreated mental illness produces socially disruptive or alarming behavior that makes him a threat to himself or others (or to himself because others become a threat to him, a la Jordan Neely). The crisis gets treated, but of course the underlying process that yields the crisis—the serious mental illness—goes untreated. An analogous thing happens in substance abuse policy, and it is part of why 100,000 people die every year from drug overdose.
Cutting through this dynamic means that you need to be able to treat someone longer term—possibly indefinitely—which requires facilities that do that. These are called “institutions for mental diseases” (IMDs), or more informally “institutions” or “asylums.” Alexander recognizes this objection and dismisses it:
If your plan is to “lock them up long-term”, keep in mind that (for now) there are almost no institutions equipped to do this. Each state usually has one center with a 3-digit number of beds for the most recalcitrant patients. Getting into these is like getting into Harvard, only in reverse - you need a spectacular anti-resume proving that you’re among the worst of the worst in the country. If you want tens of thousands of people in institutions like these, then you’ll need some kind of vast nationwide building program. Do you expect San Francisco to be good at this?
What irks me about this argument is that the lack of institutions did not come from nowhere. We used to have a lot of them. Now we have very few. That is the product of a specific policy choice: the so-called “Medicaid IMD exclusion,” which (to quote my colleagues Stephen Eide and Carolyn Gorman), “generally prohibits IMDs from billing Medicaid for care given to adults between the ages of 21 and 64 at a facility with more than 16 beds.”
The IMD exclusion has been part of Medicaid—the federal insurance program for the poor, which consequently provides many of the healthcare dollars for seriously mentally ill homeless people—since the latter became law in 1965. Its goal, as Eide and Gorman explain, was “to encourage investment in community-based, noninstitutional modes of mental health care, leave states responsible for what long-term institutionalized care would still be necessary, and control costs.” It did not, however, yield “community-based, noninstitutional modes" of mental health care. States want to shift healthcare costs on to the federal government, so if they can’t put the seriously mentally ill in institutions, they “board” them in inappropriate settings (leaving them in the emergency room, e.g.), or try to turf them as quickly as possible. No federal funding for long-term care = no long-term care.
I don’t think IMD exclusion repeal is a silver bullet for addressing disruptive mental illness, though it would almost certainly be a substantial improvement over the status quo. But the rest of Alexander’s argument rests on the idea that long-term inpatient treatment is simply not an option in most cases. He’s descriptively right, but fails to recognize that that reality is a policy choice.
Really, though, I bring up the IMD exclusion because I think the judgements which produced it are the same judgements that produce Alexander’s confusion about how to handle serious mental illness.
The title of this post is “serious mental illness is an optimization problem.” What I mean by this is that it is an attempt to find the optimal balance between two conflicting policy priorities. In this case, the priorities are the freedom of individuals to do what they please unimpeded by coercion, which is to say liberty; and the freedom of individuals not to suffer the debilitating effects of unchosen illness, which is to say health.
Alexander asks:
But okay, suppose you build those institutions. How long are you keeping people there? Remember, someone’s going to come in, start taking antipsychotics, and (if the drugs work) appear significantly saner within 2-4 weeks. Best-case scenario, they’re completely sane. Now what? Do you keep a completely sane person locked in the mental institution forever? Or do you let them out, at which point they will inevitably stop taking the drugs and become psychotic again?
The answer to the question “do you keep a completely sane person locked in the mental institution forever?” is yes, of course. For some people, the institution is the only context in which they are able to live free from profound psychosis. This strikes me as obvious. If a person will only remain sane and functional in a 24/7 residential setting, then granting him the liberty to live in the community is not merely foolish but cruel.
The fact that Alexander finds this a hard question to resolve implies that he sees the optimization problem as trying to maximize health while holding liberty constant. This is, in fact, much of what drove deinstitutionalization (of which the IMD exclusion is a part). The idea is that living in an institutionalized setting is intrinsically dehumanizing, because it deprives people of liberty. Therefore, we should discourage their use as much as possible, or even abolish them altogether.
But what if instead of trying to maximize health while holding liberty constant, we instead tried to maximize liberty while holding health constant? If instead of trying to do what we can consistent with respecting the autonomy of the sidewalk psychotic, we did whatever we needed to to keep him sane, even if it meant long-term confinement?1
My thoughts on this topic are in part influenced by the work of Neil Gong, a UCSD sociologist who has done extensive ethnographic work on mental health care in Los Angeles. (Buy Neil’s book here.) In his work, Gong compares the mental health treatment experience of Los Angeles’s seriously mentally ill homeless with that of the city’s richest denizens. Conventionally, sociologists assume that the poor are the most tightly controlled while the rich can do what they please. Gong finds that, in fact, the opposite is true. The poor are subject to a paradigm that he calls “tolerant containment”: light-touch services aimed at providing them care only insofar as it is consistent with their autonomy. The rich, by contrast, actively pay for a strategy that Gong calls “concerted constraint”: therapeutic restriction aimed at prioritizing their health over their liberty.
The paradigm that obtained after deinstitutionalization, and that inspired the IMD exclusion, and that Alexander seems to think is the best we can do, is one of “tolerant containment.” I think the fact that people pay to have their liberty taken away when they can suggests that our order of priorities is backwards.
Alexander, I assume, will object that I have not laid out a point-by-point plan for addressing serious mental illness. Doing so exhaustively would take more space than I’m willing to dedicate to this post. But the governing idea is that individuals whose serious mental illness makes them a danger to themselves or others should receive the least restrictive intervention that consistently secures their health and well-being.
What does that mean? Start with the population of interest. Alexander inaccurately claims that 22.7% of Americans have a mental illness. That’s technically true, but the population we’re interested in is those with a serious mental illness (SMI), which is 5.5%.2 The number of seriously mentally ill homeless people is smaller still. As of 2023, about 137,000 homeless people were identified as being seriously mentally ill, which is a good enough estimate for the number of bed-years you need (because people will cycle in and out of problematic mental illness).
So the question is, can and should we institutionalize an additional 140,000 people? There were about 190,000 people in inpatient psychiatric treatment in 2018,3 including about 35,000 in state hospitals and another 54,000 in private facilities. If you wanted to institutionalize 140,000 people tomorrow, that would be the equivalent of increasing inpatient treatment utilization by about 74%, restoring it to levels not seen since the 1970s.
What would that cost? In his follow-up piece, Alexander claims that a psychiatric bed costs $300,000/year. I sort of suspect this is high—this study finds the cost of treating commercially insured people with schizophrenia at about $21,000/year, and estimates like the one Alexander cites often combined fixed costs with per person costs, inflating the marginal figure. But sure, that’s about $41 billion, which is like half of what Medicaid spends on mental health generally.
I think you could maybe do this—you could end the IMD exclusion, court order every seriously mentally ill homeless person into a state psychiatric bed, and drop $40 billion a year or so to do it. But you could probably do it more cost effectively if you ended the IMD exclusion while preferring institutionalization as a method of last resort. It’s hard to construct an estimate of what percentage of the SMI homeless population would best be served by institutionalization. But I suspect some large fraction of them would be benefited by just using more aggressive supervision.
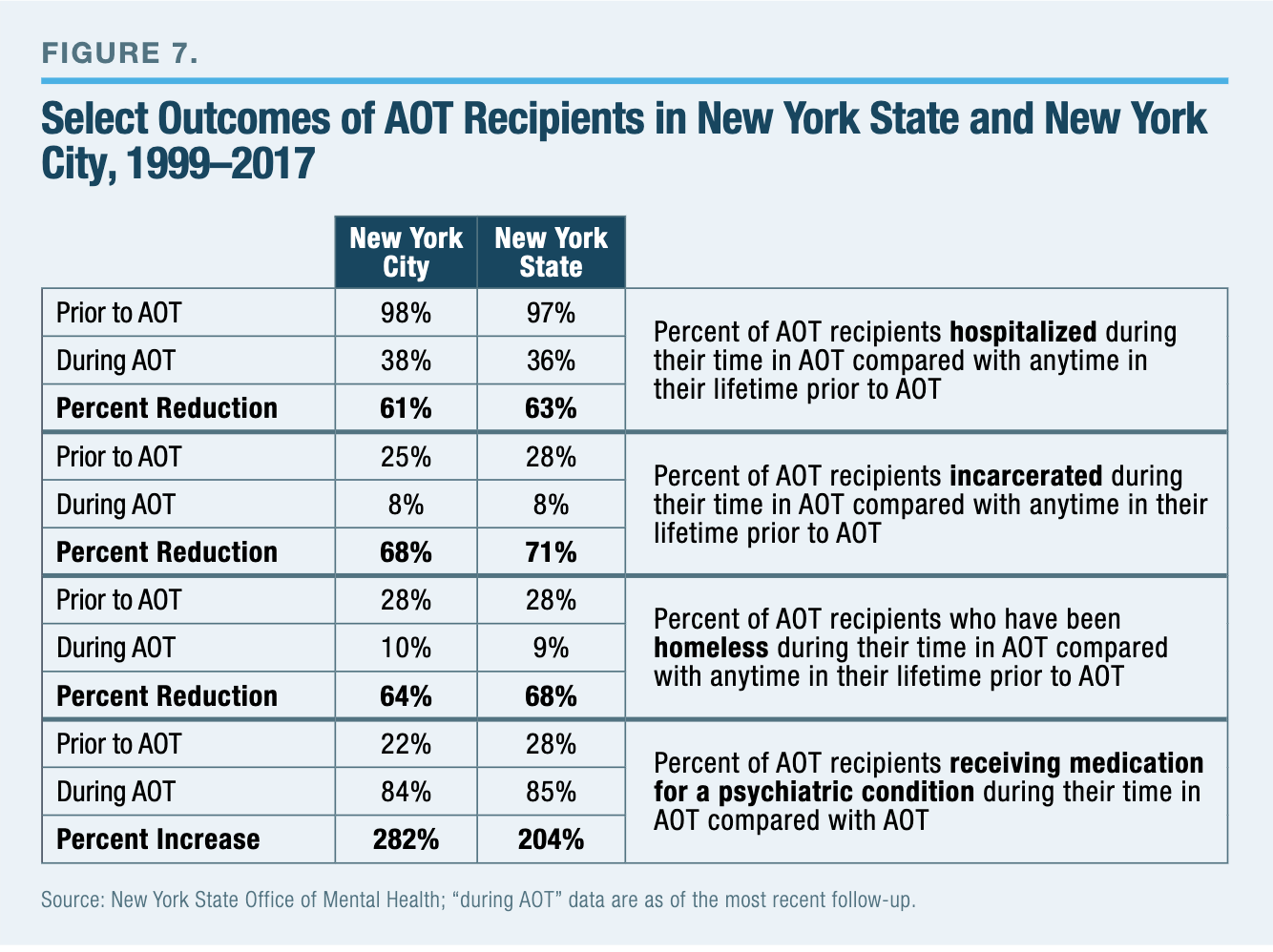
What does that mean? Court-ordered outpatient treatment is not a pipe dream—contra Alexander, who appears basically uninterested in or unfamiliar with the policy specifics. Evaluations of New York’s Assisted Outpatient Treatment law indicate that it yields significant improvements across a variety of measures, including medication compliance. Long-term supervision programs that combine regular check-ins on compliance with minor punishments for non-compliance have yielded substantial reductions in problem drinking behavior; a similar principle could apply to people under court orders to take medication. (And punishment could be mixed with reward for compliance, a la contingency management.)
Outpatient treatment is particularly viable if you lower the costs of keeping people on their meds. As Alexander himself admits, long-acting injectable formulations substantially reduce the burden of medication compliance. They are expensive, but a lot less expensive than institutionalization.
Some people will benefit from institutionalization; others can operate in the community with more supervision. Some people probably need a mix: specialized housing with services on site, permitting them some degree of freedom. Ideally, people can shift between these modalities, depending on how well they can take on the added responsibility of more liberty.
All of this is expensive. But we should recognize that the status quo is also not free. Today, cities that try at all on homelessness and mental illness deploy a patchwork of services, often redundant and overlapping, to try to keep track of an unrestricted and unpredictable population. They deal with crises, rather than causes. And I am simply not convinced that treating the former is cheaper, in the long run, than treating the latter.
This is, as promised, just a sketch. (You may note that a lot of it is shamelessly cribbed from my colleague Stephen Eide; I encourage you to read more of his work.) But the basic point is that the status quo does not do these things, and it does not do these things for reasons that are at least partially ideological: because we try to maximize liberty, rather than health. Doing it the other way would of course yield a more paternalistic system. But it would also yield a system in which both the community and — most importantly — the seriously mentally ill themselves are objectively better off.
I am actually more IMD skeptical than a lot of other people on the right. That is to say, I think many people were detained in institutions prior to the 1960s who ought not to have been there; the psychopharmacology revolution really did make a big difference; many people with disabilities can and do successfully live in the community with support; and total institutions really do create conditions with a high potential for abuse, which require careful oversight to prevent. That said, there clearly is a fraction of the mentally ill population for whom long-term, institutionalized care is appropriate, and it is a scandal that we refuse to provide it to them. (If you want an extended defense of the way that institutionalized life can be dignity enhancing, my colleague John Hirschauer writes more persuasively about it than I ever will.)
Sort of like how he doesn’t seem to know about the IMD exclusion, the fact that Alexander just uses the AMI number instead of the SMI number leads me to wonder how firm of a grasp he actually has on mental health policy.
I use the 2018 figures because beds were dramatically reallocated in 2020 due to COVID.
I like this piece, but lurking in the background of all of this is America's absurdly strong system of judicial review. Some judge somewhere would find fault with every single policy prescription listed here and block it- then the issue would be tied up in court for years if not longer. It's very under-discussed how our current problems with homelessness all stem from judicial review- court decisions in the 70s that blocked panhandling & vagrancy laws, court decisions that made institutionalization much more difficult, and so on all the way up to Grants Pass. I've grown much more skeptical about judicial review in recent years, especially the power of 1 local judge to block literally anything they choose to, and I think that part of the solution is paring back the power of the judiciary
Deinstitutionalisation happened more or less everywhere but the outcomes you describe occurring in America with respect to people with serious mental illness (SMI) didn’t happen everywhere, ergo, deinstitutionalisation is not the problem nor re-institutionalisation the answer. In the UK we have community treatment orders (CTO) for non-compliant (and potentially risky) SMI patients and such patients are usually prescribed long-acting intra-muscular anti-psychotics. If they disengage and become non-compliant with treatment, they can be recalled to hospital.